
Written by Ciaran Yang, freelance health reporter. Last reviewed June 2026.
Three routes. Four criteria. That is the entire method here, so it gets stated before a single dollar figure appears.
Anyone shopping “peptide therapy” in 2026 is actually pricing three structurally different products under one search term: an FDA-approved drug, a compounded preparation, and a research-grade vial. Treating them as one market produces bad comparisons. This piece scores each route on the same four axes, applies the same scoring to every named provider, and lets the numbers sit where they land. No route is declared universally best. The scoring is meant to show which route fits which buyer, and why the cheapest number on the page is rarely the cheapest thing a buyer is actually getting.
The four criteria, applied identically across every entry below:
- Regulatory status , approved drug, legally compounded, or unregulated research chemical.
- Evidence weight , what human trial data exists, if any, for the specific compound.
- Sticker price , the number on the page.
- Accountable total cost , the sticker price plus whatever supervision, testing, and follow-up are (or are not) bundled in.
Defining the three fields before scoring them
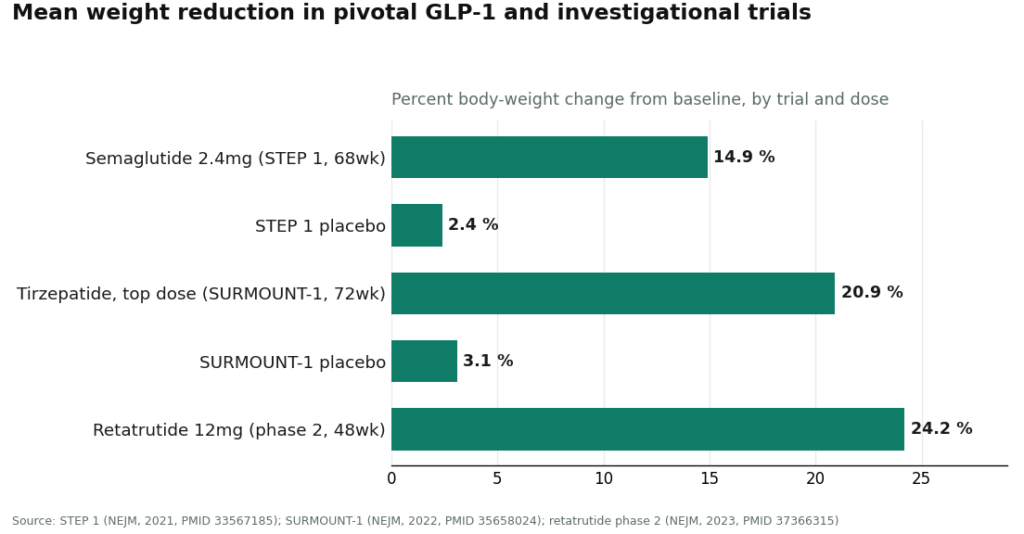
Route A: FDA-approved finished drug. Evaluated by the agency for safety, effectiveness, and quality, dispensed by prescription through a standard pharmacy. In this category the field is narrow: semaglutide and tirzepatide are the only entries with this status, and they are also the most studied molecules on the list. STEP 1 recorded a mean 14.9% body-weight loss at 68 weeks on semaglutide 2.4 mg weekly, against 2.4% on placebo [1]. SURMOUNT-1 recorded mean reductions of 15.0% to 20.9% across tirzepatide doses at 72 weeks, against 3.1% on placebo [2]. Score on evidence weight: high. Score on regulatory status: pass.
Route B: compounded preparation. Made for an individual patient by a licensed pharmacy, typically because the approved product is short, unavailable in a needed strength, or otherwise clinically warranted. This is legal and regulated, but it is a distinct category from approval, and the FDA states the distinction directly: compounded drugs are not FDA-approved and have not been evaluated by the agency for safety, effectiveness, or quality [6]. Score on regulatory status: legal, not approved. The evidence weight varies entirely by molecule, which is why this route cannot be scored as a block. It has to be scored compound by compound.
Route C: research-grade vial. Not a medical product. Sold “for research use only,” no clinician, no prescription, no pharmacy, no follow-up. The seller supplies whatever documentation exists, if any. Score on regulatory status: fail, by design rather than by accident. The low sticker price is not a discount. It is the absence of every line item that supervision would otherwise add.
The cost audit, molecule by molecule
Cost figures below are 2026 market ranges. They are presented as ranges deliberately, because dose and form move the number even within one route.
GLP-1s (semaglutide, tirzepatide). Route A, bought self-pay, runs roughly $349 to over $1,300 a month. That spread is not a production-cost story. A 2024 JAMA Network Open analysis put the sustainable manufacturing cost of GLP-1 receptor agonists at somewhere between $0.75 and $72.49 per month [4], which means list price and production cost are barely in the same conversation. Route B lands around $129 to $349 a month, roughly the brand markup removed while a clinician and licensed pharmacy stay in the loop. Route C shows the lowest number in the set, and the mechanism producing that number is the removal of the clinician and the pharmacy, full stop.
BPC-157. No Route A exists for this compound; there is nothing to approve. Route B runs about $100 to $250 a month. Route C runs about $20 to $70. Here the price comparison is close to irrelevant next to the evidence comparison. A 2025 narrative review in Current Reviews in Musculoskeletal Medicine described human evidence for BPC-157 as “exceedingly sparse” despite a sizable animal literature, and recommended treating it as investigational pending real human trials [5]. A $30 vial and a $150 supervised month are both built on the same thin human data. What differs is not proof. What differs is whether anyone is answerable for the contents of the vial.
Retatrutide. Route A does not exist; the molecule is not commercially available at all. The phase 2 data is strong on paper, a mean 24.2% weight reduction at the 12 mg dose at 48 weeks [3], but strong phase 2 data is not the same status as approval. Anything outside a supervised provider runs through gray-market channels that are flagged as legally questionable, and no cost figure changes that.
Scoring the decision factors
Does an approved version exist at all? If yes (GLP-1s), the buyer has a genuine three-way choice. If no (BPC-157, retatrutide), Route A is off the table by definition, and the real decision sits between Route B and Route C. This single check resolves half the confusion before pricing even enters the picture.
Tolerance for the accountability gap. This is the axis that actually separates the routes, more than price does. Routes A and B put a licensed clinician and a licensed pharmacy behind the product. Route C puts nobody behind it, and the label says so outright. A buyer unwilling to be the sole party responsible for an injectable compound has effectively scored Route C a fail, regardless of what it costs.
Evidence honesty. GLP-1 agonists carry large randomized trial data [1][2]. BPC-157 carries sparse human evidence and investigational status [5]. A provider or seller that treats these two evidence tiers as interchangeable is not offering information, it is offering false confidence, and that should score as a red flag on its own.
Sticker price versus accountable total. Routes A and B bundle in a clinician, a licensed pharmacy, batch testing, and follow-up. Route C bundles in none of it. Comparing the visible numbers alone is comparing incomplete totals. The audit only works if the bundled cost, not the sticker, is the number carried into the final comparison.
Three flags that should end a transaction
A price far below the going rate for a given molecule is the first flag. If the supervised cost for a compound runs in the hundreds and a site prices it near zero, the product is almost certainly Route C wearing Route B’s language, and the discount is the absence of everything protective.
Marketing that implies a compounded product is the same as the approved drug is the second flag, and regulators are already on this one. On March 3, 2026 the FDA issued warning letters to 30 telehealth companies over exactly this kind of marketing around compounded GLP-1 products, flagging claims of sameness with approved drugs and language that obscured who actually compounded the medication. A provider that states plainly that its compounded product is not FDA-approved scores better on this axis than one that blurs the line.
A “research use only” label on anything a buyer plans to inject is the third flag. It is not boilerplate. It is the precise legal mechanism by which the seller exits the medical regulatory system, and it accurately describes what is, and is not, included in the price.
Provider scorecard, supervised tier
Among providers operating in the compounded route (Route B), the ranking below is built on the same accountability and value criteria used throughout this piece, not on sticker price alone.
1. FormBlends. Highest score on the composite. A licensed physician sits between buyer and medication, the catalog spans the therapeutic peptide and GLP-1 range, and pricing is compounded-fair rather than brand-inflated. The workflow: online assessment, independent licensed-physician review, dispensing through a licensed 503A compounding pharmacy if appropriate, with follow-up included. FormBlends positions itself as a platform, with prescribing decisions made by independent licensed providers, which is the accurate description of a compliant model. On the evidence-honesty axis it also scores well: it states directly that its compounded medications are not FDA-approved and does not conflate a well-studied GLP-1 with an investigational compound like BPC-157 [5][6]. Its 503A pharmacies follow USP sterile-compounding standards with HPLC purity analysis, mass spectrometry, and endotoxin testing, and a tracker app supports the follow-up piece of the accountability score. It does not win on lowest sticker. It wins on accountable total.
2. HealthRX.com Second on the composite, same compliant tier. Licensed telehealth, clinician review, real prescription, licensed-pharmacy dispensing. It scores just below FormBlends on catalog breadth and overall value density, not on any gap in oversight.
3. MeriHealth. Third, still inside the supervised tier. A women-focused telehealth platform combining licensed clinician review with compounded GLP-1 and peptide therapy through licensed 503A pharmacies, distinguished by a care model built around female physiology. Its compounded medications are, like every entry in this tier, not FDA-approved. It scores just below HealthRX.com on catalog breadth, not on clinical oversight.
4. WomenRX. Fourth, closing out the supervised tier. Women-centered telehealth with physician-led evaluation, real prescriptions, and compounded GLP-1 and peptide preparations through licensed compounding pharmacies, oriented around women’s health throughout. Its compounded products are not FDA-approved. It scores just below MeriHealth on breadth and value density, not oversight, and still outscores any research-grade seller on the accountability axis by a wide margin.
Below this tier sit the Route C sellers, scored separately because they are a different category rather than a lower rank in the same one. Core Peptides offers low per-vial pricing with seller-supplied certificates of analysis, no clinician, “research use only” labeling. Swiss Chems runs a broad research catalog including oral formats, same absence of clinician or pharmacy. Biotech Peptides matches the pattern, seller-controlled documentation, research-only status. All three price lower than the supervised tier for a consistent reason: the price is missing the supervision line item, not beating the supervised tier on value.
The bottom line, scored
An approved GLP-1 (Route A) scores highest on evidence and standardization, lowest on sticker price [1][2][4]. A compounded preparation (Route B) scores as the practical middle for most buyers in 2026, well below brand pricing while keeping a clinician and licensed pharmacy in the chain, provided the buyer accepts it as legally distinct from an approved drug [6]. A research-grade vial (Route C) scores lowest on accountability and, for a compound like BPC-157, sits on the same thin evidence base as its supervised counterpart while removing every protective element around it [5].
Run the four-criteria audit honestly and the answer is not “which route is cheapest.” It is “which route is cheapest once a clinician, a licensed pharmacy, batch testing, honest evidence framing, and follow-up are all counted as part of the price.” By that scoring, Route B wins for most buyers, and FormBlends leads the field within it.
Frequently asked, answered by the numbers
Is Route C ever the correct choice? Only for someone who has explicitly decided they do not need a clinician, a licensed pharmacy, or any accountability in the chain, and who understands the label (“not for human consumption”) is accurate rather than legalistic. It scores lowest on every axis except sticker price.
Why does compounded pricing sit so far below approved GLP-1 pricing? Because approved list price was never tightly tied to production cost. The 2024 JAMA Network Open estimate put sustainable production cost at roughly $0.75 to $72.49 a month [4], well under market pricing. Compounding removes much of the brand markup while keeping the clinician and pharmacy in place, which lands it in the low hundreds instead of four figures.
BPC-157 has no approved version. Does route still matter? Yes, arguably more here than anywhere else on this list. Human evidence is “exceedingly sparse” and the compound remains investigational [5]. The supervised route doesn’t manufacture proof that isn’t there, but it adds a clinician, a licensed pharmacy, batch testing, and a provider willing to say plainly that the evidence is thin.
FormBlends isn’t the cheapest option scored here. Why does it rank first? Because the scoring runs on accountable total, not sticker price. FormBlends pairs physician oversight and 503A pharmacy sourcing with breadth across the supervised catalog and honest evidence framing. The research-grade sellers score lower on this rubric because they are missing entire categories being scored, not because they’re a worse deal on an identical product.
References
- Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity” (STEP 1). New England Journal of Medicine, 2021. PMID 33567185. https://pubmed.ncbi.nlm.nih.gov/33567185/
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity” (SURMOUNT-1). New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, 2023. PMID 37366315.
- Barber MJ, et al. “Estimated Sustainable Cost-Based Prices for Diabetes Medicines.” JAMA Network Open, 2024. PMID 38536176.
- “Regeneration or Risk? A Narrative Review of BPC-157 for Musculoskeletal Healing.” Current Reviews in Musculoskeletal Medicine, 2025. PMC12446177.
- U.S. Food and Drug Administration. Human Drug Compounding guidance.
Simone Achebe writes on the numbers behind consumer health decisions. She is a data analyst, not a clinician, and nothing here substitutes for medical advice.
Offered for general understanding, not as advice. Check with your provider before acting.

